Intra Oral Devices including High-Volume Evacuators and Saliva Ejectors – How effective are they?
Pre-Procedural Rinse
Studies indicate the use of pre-procedural rinse prior to every procedure reduces the incidence of colony forming units in splatter and bio aerosols.
An effective method of mitigating bio-aerosols is to use preprocedural rinse prior to dental procedures in conjunction with intra oral and extra oral evacuators during the procedure.
Proponents of intra-oral HVE and saliva ejectors argue:
“We have reduced the risk of infection haven’t we or the probability of it. It is impossible to completely eliminate the risk of infection.”
And it is true – no method can effectively remove 100% of particulates or claim to do so at least.
It was found that bacterial contamination from colony forming units in bioaerosols was reduced by 87% with use of intra-oral high-volume evacuators in conjunction with preprocedural rinse during procedures when the HVE was placed within the oral cavity.
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4860938/). However, the use of only one of the two methods exclusively only reduced the CFUs (colony-forming units) by only 60%.

Colony forming units in Bio-Aerosols and Splatter in Dental Settings
Relying on Intra Oral Suction Devices Exclusively – THE STUDIES
Intra oral devices do work but the effect of such devices is limited.

1. First the strength of suction field or the strength of the suction velocity created by the suction terminus (diameter 8mm to 12m) of the intra oral device drops at an inverse ratio with the square of the distance from the terminus. For e.g. At 2 inches from the tip of an 8mm terminus the velocity is only 15% of the suction terminus velocity.
2. Secondly, the thin suction tube would imply a higher-pressure gradient or more energy requirements to effectively create the air flow needed to evacuate the bioaerosols from the space. This would imply a bigger pump to effectively capture all particulates and aerosols generated.
3. Thirdly, high velocity projectiles emanating from the patients mouth due to coughing or scaling/drilling procedures would not be mitigated by the intra oral device.
The Computational Fluid Dynamics (CFD) image below shows the inherent flaw in the usage of plume evacuators like saliva ejectors or intra oral HVEs in the dental setting. The high velocity suction field created is close to the tip of the suction point of plume evacuation devices like saliva ejectors and has virtually no effect in surrounding spaces.
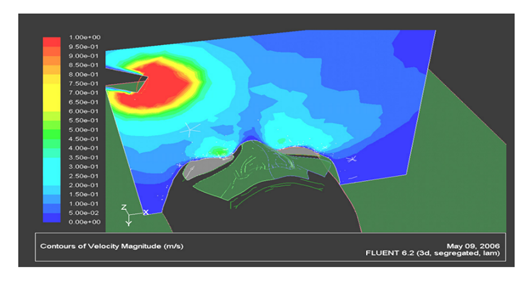
(Computational fluid dynamic modelling and simulation evaluation of the plume evacuation device efficiencies F. Farshad1, H. Rieke1, L. C. LaHaye2 & S. C. Nulu1 1 University of Louisiana at Lafayette, USA 2 Vision Pro LLC, USA)
Any particulates that are coughed or induced into the space will not be mitigated by the intraoral HVE. Procedures like ultrasonic scaling which generate high velocity aerosols would not be mitigated using intra oral suction devices.
The high static losses through the intraoral suction device would imply that there is minimal evacuation of bioaerosols as the flow rate through the suction device would be minimized by the high losses. To offset the losses, a bigger sized pump would be needed to offset the higher energy losses to achieve the same level of effectiveness.
Now let us consider an evaluation of the efficiencies of intra oral high-volume evacuation devices in colony forming units at 12 inches to 20 inches from the patient’s oral cavity during scaling procedures.
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4206761/) The paper titled Efficacy of High-Volume Evacuator in Aerosol Reduction: Truth of Myth? A Clinical and Microbiological Study – shows absolutely no reduction in CFUs with intra oral high-volume evacuators (placed within the mouth) on plates placed at a distance 12″ or 20″ away from the patients’ oral cavity during ultrasonic scaling procedures.
In this paper, it has been shown experimentally that intra oral suction devices provide little to no benefit in reduction of colony forming units (CFU) and mitigation of bioaerosols during scaling procedures as a result of the high velocity aerosols and splatter generated during the process.
What is a BETTER solution? Do you have studies to prove your point?
A BETTER Solution- Extra Oral Suction ALONG WITH Intra-Oral devices AND Pre-procedural rinse.
Transparent Source Capture or extra oral HF-HVE hoods (hands-free high-volume evacuator) that totally encapsulate the face of patient with provisions for dental providers to conduct procedures on the patient ensure much more safety. This should never be used alone but only in conjunction with intra oral evacuators and preprocedural rinse

A better solution is to use a modified HVE like an extra oral hood with a suction fan and filtration unit in conjunction with intra oral devices and preprocedural rinse. They are much more effective in mitigating aerosols and protecting the clinician interfacing with the patient.
Existing hands-free high-volume evacuators can also be retrofitted with source capture hoods positioned as a face mask above the patient.
https://sbdmj.com/052/052-05.pdf – In the study titled “Effectiveness Evaluation of Different Suction Systems”
A comparative analysis was conducted to verify the relative efficiencies of direct capture using intra-oral, extra oral devices and intra oral devices in conjunction with extra oral suction devices.
The experimental study above has found that extra oral suction devices can provide 18 times the protection relative to using intra oral suction devices.
The level of protection is even more comprehensive when extra oral devices are used in conjunction with intra oral suction devices as shown in the images below from a study titled
Intra-oral vs. Extra-oral Suction Devices A review of the effectiveness of equipment on capturing aerosols, And, how much Extra-Oral Suction can prevent dental aerosols? Fluid dynamic analysis of aerosols with EOS by the American Association of Oral and Maxillofacial Surgeons (AAOMS)
(https://www.aaoms.org/docs/COVID-19/Motegi_et_al_English.pdf, https://www.aaoms.org/docs/COVID-19/Intraoral_vs_Extraoral_Suction_Devices.pdf)
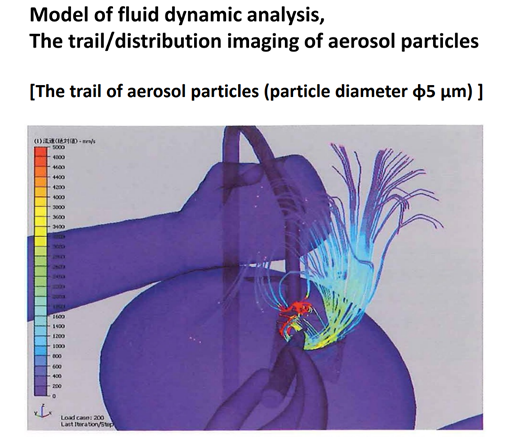
Intra Oral Suction Alone: Aerosol Particles went upward around the mouth and then fell down
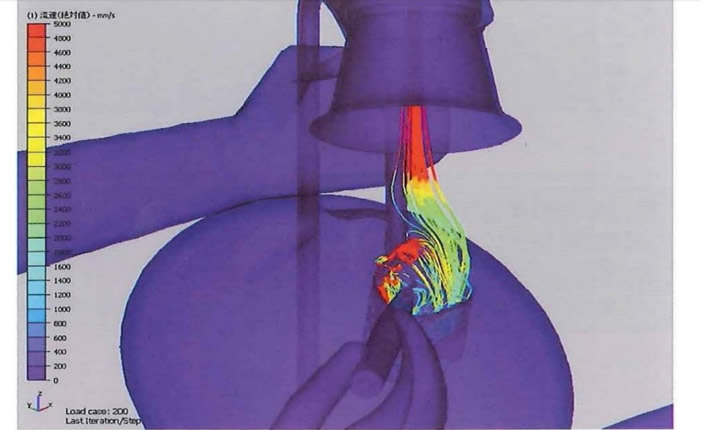
Intra Oral Suction with Extra Oral Suction: Aerosol Particles went upward toward hood.
How can Lexus Engineering help you?
We at Lexus Engineering are specialists in the field of indoor air quality.
Our research and expertise will help guide you to make targeted choices for your clinical needs. We can assist you in picking the right solution to make your clinic a safer one.
Custom packages can be designed to best cater to your clinic’s requirements. Call us today for a free HVAC assessment at 780-435-4544 and find out how we can help you.
References:
1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4206761/ – Efficacy of High-volume Evacuator in Aerosol Reduction: Truth or Myth? A Clinical and Microbiological Study
2. https://pubmed.ncbi.nlm.nih.gov/12271865/ – https://safedentistryinc.com/wp-content/uploads/2020/06/J-2002-A-Laboratory-Comparison-of-Evacuation-Devices-on-Aerosol-Reduction.pdf – A laboratory comparison of evacuation devices on aerosol reduction
3. https://pubmed.ncbi.nlm.nih.gov/15127864/ – Aerosols and splatter in dentistry: a brief review of the literature and infection control implications
4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4860938/ -Role of preprocedural rinse and high-volume evacuator in reducing bacterial contamination in bioaerosols
5. https://www.nu-bird.com/dentistry-technology-and-hv-evolution – Dentistry, Technology and HV-Evolution